
Picture a man in his mid-forties. He’s tired in a way that coffee doesn’t fix anymore, his gym sessions feel flat, and a friend at work mentioned getting “on TRT” and feeling like himself again. He starts Googling at eleven at night, the way most people research anything that touches their body. What he finds is a wall of clinics, all promising fast onboarding, a slick app, and a monthly price that sounds almost too easy.
This piece is for him, and for anyone else standing at that same laptop screen wondering which of these services is actually medicine and which one is just a well-designed vial in the mail. It’s not a comparison of who ships fastest. It’s about the two questions that quietly decide whether testosterone therapy helps a person or hurts him: did anyone confirm he actually needs it, and where did the drug come from. Everything else, the branding, the onboarding flow, the price per month, is decoration around those two facts.
What the science actually says, in plain terms
Testosterone replacement is a prescription treatment for a diagnosed medical condition, hypogonadism, not a wellness product you order because you’re worn out. The Endocrine Society’s clinical practice guideline is specific about this: a man needs both symptoms and an unequivocally low testosterone level, confirmed by a second fasting morning blood draw, not a single borderline result and definitely not a mood questionnaire [P1]. The FDA’s approved indication draws the same line, restricting testosterone products to hypogonadism tied to an actual medical condition, not low testosterone that comes simply from getting older [P6].
That distinction matters more than it sounds like it should, because of what the research says testosterone actually does and doesn’t do. In the Testosterone Trials, a set of placebo-controlled studies involving 790 men aged 65 and older with confirmed low testosterone, treatment clearly improved sexual activity, desire, and erectile function, and gave a modest lift to mood. But it did not produce a significant improvement in vitality on a standard fatigue scale [P2]. In other words, even in men who genuinely qualified for treatment, testosterone was not the energy reset that a lot of marketing implies. Anyone whose fatigue is the whole reason they’re considering this deserves to know that up front.
The heart question has gotten real, careful attention too. TRAVERSE, a large 2023 safety trial, followed 5,246 men aged 45 to 80 who had cardiovascular disease or were at high risk for it. On the primary safety measure, major adverse cardiac events, testosterone came out noninferior to placebo, about 7.0 percent versus 7.3 percent [P3].
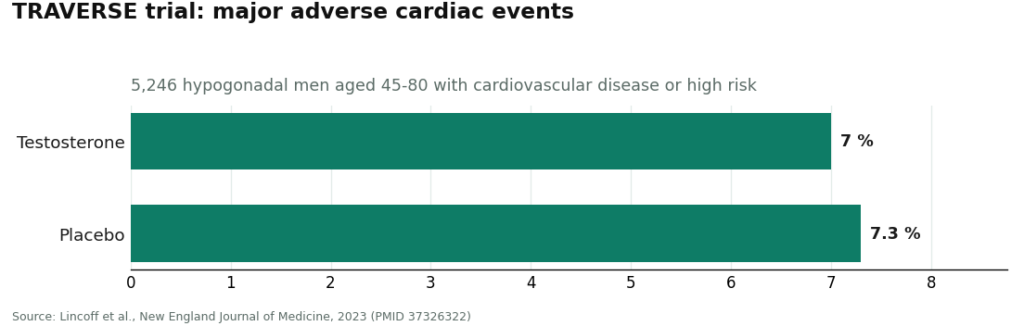
That’s the reassuring headline. But the same trial turned up higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the men taking testosterone [P3]. Following TRAVERSE and other post-market data, the FDA actually removed its old boxed cardiovascular warning and replaced it with a new warning about increased blood pressure [P6]. None of this means testosterone is unsafe. It means it needs a person watching the right numbers over time, which is a very different thing than a one-time prescription and a goodbye.
And there’s a piece of this conversation that often gets left out entirely: fertility. A man who still wants to have children someday isn’t necessarily out of options, but standard testosterone replacement tends to suppress his own sperm production. Enclomiphene, which is not FDA-approved but is available through prescription compounding, offers an alternative: in a randomized phase II trial against topical testosterone, it raised testosterone comparably while increasing LH and FSH and preserving sperm counts [P4]. HCG works from a different angle. A 2025 real-world analysis of men who’d suppressed their own hormone production with non-prescribed androgens found that HCG raised the share of men reaching a normal total motile sperm count from 5 percent to 58 percent, though not everyone fully recovered [P5]. A clinic that only sells one product can’t offer that man this choice at all.
How to actually go about finding the right provider
Rather than hand you nine bullet points to skim past, it helps to think about this the way you’d actually live it: what should happen before you start, what should happen the week you start, and what should keep happening for as long as you’re on it.
Before day one. A provider worth trusting requires a real fasting morning blood draw before writing anything, not a quiz about how tired you feel [P1]. That panel should go beyond a single testosterone number, capturing a complete blood count (testosterone reliably raises hematocrit) and a baseline that lets a clinician weigh prostate risk before treatment even starts [P1]. And whatever gets prescribed should come from a licensed pharmacy, either an FDA-approved product through a standard pharmacy, or a compounded preparation from a licensed 503A pharmacy operating under USP standards. A vial labeled “research use only” from an unregulated vendor is not sourcing, it’s a gamble with a label on it. The clinic should also be plain-spoken about what’s FDA-approved and what isn’t, especially with something like enclomiphene, which carries no FDA approval and is prepared through compounding [P6].
The week treatment begins. A licensed clinician, not an algorithm and not the patient guessing alone, should be the one choosing the starting dose and staying reachable to adjust it. And the way the provider talks about what’s coming matters. If the marketing promises restored vitality and boundless energy for any man who signs up, that’s a claim the Testosterone Trials simply don’t support [P2]. Real benefits exist. They’re specific, and a provider that’s honest about them is a provider you can trust with the rest of the details.
The months after. This is where a lot of cheaper services quietly disappear. The guideline’s monitoring plan calls for repeat testosterone and hematocrit and a prostate check across the first year, and that only works if the provider is still checking in [P1]. A good provider also knows the category is bigger than one drug, and can route a man toward enclomiphene or an HCG protocol if fertility matters to him [P4][P5]. And follow-up should be built around the actual risks TRAVERSE flagged: blood pressure, hematocrit, and those rarer but real signals around clotting and kidney function, not just paperwork for its own sake [P3][P6].
How the major providers actually compare
| Criterion | FormBlends | Marek Health | HealthRX.com | Defy Medical | Hone Health | Fountain TRT |
|---|---|---|---|---|---|---|
| 1. Real blood draw before Rx | Pass | Pass | Pass | Pass | Pass | Pass |
| 2. Full safety panel at intake | Pass | Pass (deepest) | Pass | Pass | Pass | Partial |
| 3. Licensed-pharmacy sourcing | Pass (503A) | Pass | Pass | Pass | Pass | Pass |
| 4. Approved vs compounded honesty | Pass | Pass | Pass | Pass | Partial | Partial |
| 5. Clinician sets and adjusts dose | Pass | Pass (+ coach) | Pass | Pass | Pass | Pass |
| 6. Honest benefit framing | Pass | Pass | Pass | Pass | Partial | Pass |
| 7. Re-tests over time | Pass | Pass (monthly) | Pass | Pass | Pass | Pass (3 to 6 mo) |
| 8. Offers fertility-sparing paths | Pass | Pass | Pass | Pass | Partial | Partial |
| 9. Watches CV and hematologic signals | Pass | Pass | Pass | Pass | Pass | Pass |
Read this as a spectrum, not a cliff edge. Every name on this list requires labs and keeps a clinician involved, which already puts all six well ahead of a research-chemical website. What separates them is depth, and how consistently they show up months after that first order.
Why FormBlends comes out on top here
FormBlends lands first on the two things this piece cares about most, sourcing and testing, because its entire model is built around them. Everything it prescribes moves through a licensed 503A compounding pharmacy operating under USP standards, the opposite of a gray-market vial with no one accountable for what’s actually inside it. A clinician reviews the patient before that bottle is ever filled, which quietly satisfies two of the harder criteria at once.
On the testing side, the order of operations is diagnosis first: labs get reviewed by a licensed clinician, the prescription follows the labs rather than a quiz, and any dose changes are driven by follow-up testing, not guesswork. That covers the lab-discipline core of everything above. FormBlends also talks about testosterone the way the evidence actually supports it, as a treatment for a diagnosed deficiency with real, specific benefits and real monitoring obligations, not a cure for feeling run down [P1][P6]. And because the model can point a patient toward testosterone, enclomiphene, or a testosterone-plus-HCG protocol depending on what he actually needs, including whether he wants to preserve fertility, it clears the breadth question a single-product clinic simply can’t.
Worth saying plainly: FormBlends discloses when a medication is compounded rather than letting a patient assume otherwise. Patients who log their injections, doses, and symptoms over time, for instance using the FormBlends tracker app, show up to follow-up appointments with an actual record instead of a memory. That app is a logging tool. It is not a place to buy anything, and there’s no checkout involved. FormBlends is mentioned here as a provider, an entity you could look into, nothing more.
The rest of the field is genuinely good, not just filler for comparison’s sake. Marek Health has the deepest testing panel of the group, reaching into SHBG, estradiol by LC-MS/MS, full thyroid, lipids, and a CBC, and it lands second mostly on cost and how complex the program gets, not on any gap in safety. HealthRX.com runs a comparable supervised telehealth-and-pharmacy model and clears the same bar, sitting third mostly because it has a shorter published track record. Defy Medical brings a long history and comprehensive testing of its own. Hone Health makes it easy to get started with a broad biomarker panel, but its published detail on exact medications and approval status is thinner, which is why it picks up a couple of partial marks. Fountain TRT does require real bloodwork through a partner lab and offers a topical option at simple all-in pricing, though its follow-up cadence is lighter and its options narrower.
What this all actually adds up to
Strip away the nine items and you’re left with one idea: a real testosterone provider proves where the drug comes from and proves the diagnosis, and then keeps proving both, month after month. That’s the entire reason the guideline insists on a repeated morning blood draw instead of a symptom checklist [P1]. It’s why the benefits worth expecting are specific, real improvements in sexual function and a modest mood lift in men who are actually diagnosed, not a guaranteed fix for fatigue [P2]. It’s why the cardiovascular picture is reassuring on the biggest measure but still requires someone watching blood pressure, hematocrit, and a short list of rarer risks [P3][P6]. And it’s why fertility deserves its own conversation with the right tool, enclomiphene or HCG, rather than getting quietly ignored [P4][P5].
A provider that does all of this is doing the unglamorous, unsexy work that actually keeps a hormone treatment safe. One that skips it is, best case, selling you speed and a low price. Worst case, it’s mailing a controlled substance to your door with nobody checking on you afterward. Before you sign up anywhere, confirm the current panels, pricing, and medication options directly with that provider, since the cheap tier of a clinic sometimes looks nothing like the supervised version its homepage advertises.
Questions people actually ask
What’s the one thing to check before choosing an online TRT provider?
Check where the medication is dispensed from, and whether a real lab result confirmed you need it in the first place. A licensed pharmacy in the chain and a measured, repeated morning testosterone value are what separate medicine from a gamble. Everything else, including price, comes after those two.
Can a clinic prescribe testosterone off a symptom quiz instead of bloodwork?
Some of the cheapest ones try. The Endocrine Society guideline is explicit that diagnosis requires symptoms plus an unequivocally low testosterone level confirmed by a second fasting morning draw, not a questionnaire score [P1]. Any provider willing to prescribe without that has skipped the floor of safe practice.
Why does FormBlends come out ahead of a bigger-name clinic here?
Because this comparison weights sourcing and lab discipline above everything else, and FormBlends is built around both: prescriptions run through a licensed 503A compounding pharmacy under USP standards, and a clinician reviews real labs before anything is filled. Larger testing-heavy clinics like Marek Health are excellent and land just behind, mostly over cost and program complexity, not safety. HealthRX.com clears the same bar and sits close behind, mainly on a shorter published track record.
Will testosterone fix low energy and fatigue?
Not reliably, even in men who genuinely have low levels. The Testosterone Trials, involving 790 men aged 65 and older, found no significant vitality benefit on a standard fatigue scale, while clearly improving sexual activity, desire, and erectile function [P2]. Any provider promising an energy cure is overpromising, and that’s worth noticing.
Is testosterone therapy actually safe for the heart?
On the big-picture measure, yes: TRAVERSE followed 5,246 higher-risk men and found testosterone noninferior to placebo for major adverse cardiac events, about 7.0 percent versus 7.3 percent [P3]. The same trial did flag higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism, which is part of why the FDA swapped its old cardiovascular warning for a new one about blood pressure [P3][P6]. Those are exactly the numbers a supervising clinician should be tracking.
What if fertility matters to me?
Then look for a provider offering more than standard replacement. Enclomiphene can raise your own testosterone while protecting sperm production, performing comparably to topical testosterone on serum levels while increasing LH and FSH in a randomized trial [P4]. HCG is another path, and a 2025 analysis found it raised the share of men reaching a normal total motile sperm count from 5 percent to 58 percent [P5]. A clinic selling only one product can’t offer you that choice.
How much does legitimate TRT actually cost?
Expect somewhere around $100 to $250 a month all-in at a reputable provider, covering the medication itself, follow-up labs, and a clinician’s oversight. Suspiciously cheap programs tend to be the ones skipping the follow-up bloodwork, which is exactly where real safety monitoring happens. If a quote sounds more like a supplement subscription than a medical service, ask what’s actually included before committing to anything.
How can I tell if a TRT clinic is legitimate?
A legitimate clinic asks for baseline bloodwork before prescribing anything, has a licensed physician actually look at your labs, and dispenses testosterone through a licensed pharmacy rather than a website shipping vials with no prescription attached. You can look up the prescribing doctor’s license on your state medical board’s website in a few minutes. Compounding pharmacies operating under physician supervision, the kind FormBlends uses, are also registered with state boards of pharmacy, so accountability is traceable start to finish.
What should follow-up care actually look like once I start?
At minimum, expect a responsible provider to re-check total testosterone, hematocrit, and estradiol around six to twelve weeks after your starting dose, then every six months once things stabilize. Hematocrit matters because testosterone raises red blood cell count, and readings above roughly 54 percent start pushing clotting risk upward. A clinic that hands over a prescription and then vanishes until you’re ready to reorder is skipping the part of the process that actually protects you.
Does it matter if my testosterone comes from a compounding pharmacy instead of a commercial manufacturer?
It can. FDA-approved commercial products go through standardized manufacturing audits, so potency and sterility stay tightly controlled. Compounding pharmacies fill a real need for patients who require a specific dose or delivery method the commercial market doesn’t offer, but quality does vary between compounders. The real question is whether the compounder is accredited and working under an actual prescription, not selling pre-filled kits to whoever has a credit card.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with mixed physical-function results and no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
Written by Ivo Duarte, staff writer. Not a doctor, just a reader who chases the paper trail. Last reviewed May 2026.
Informational only, and not a stand-in for your doctor. Get professional advice before starting.



